MTHFR Gene Explained: What Your Variants Actually Mean
The MTHFR gene is one of the most talked-about — and most misunderstood — topics in consumer genetics. Here's what the science actually says about C677T, A1298C, and your health.
Key Takeaways
- MTHFR is an enzyme that converts folate into its active form (5-MTHF) — common variants C677T and A1298C reduce efficiency but do not stop the enzyme from working
- Only the homozygous C677T genotype (TT) has a consistently demonstrated clinical effect on folate metabolism and homocysteine levels — heterozygous carriers usually have little measurable health impact
- For TT carriers with confirmed elevated homocysteine, switching from folic acid to methylfolate supplementation is a reasonable, evidence-supported option to discuss with your doctor
- Most MTHFR myths online dramatically overstate the risks — major medical organizations do not recommend routine MTHFR screening for the general population
- DNA Explore checks your C677T and A1298C genotypes from existing 23andMe or AncestryDNA raw data, processed entirely in your browser
“I signed up for 23andMe in 2017 because I was fascinated by what my DNA could tell me. Six years later, my data was compromised in their breach — I'm a confirmed class member in the litigation. I didn't want to hand my genetic data to another company, so I built a tool where everything stays on your device. Then I thought: why not give people what I was actually searching for when I got my DNA tested in the first place — actionable health insights, drug metabolism analysis, risk scores — things you can actually do something with.”
What the MTHFR Gene Actually Does
From Folate to Methylation
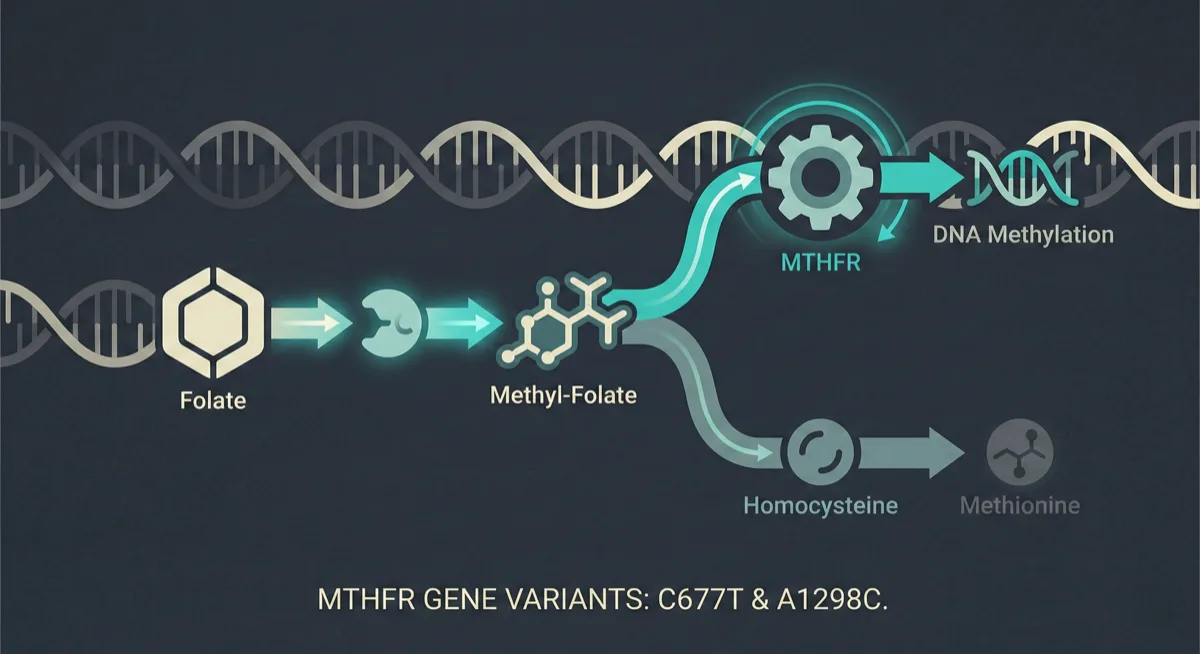
MTHFR stands for methylenetetrahydrofolate reductase — an enzyme your body uses to convert folate (vitamin B9) into its active form, 5-methyltetrahydrofolate (5-MTHF). This active folate is essential for a biochemical process called methylation, which plays a role in DNA synthesis, neurotransmitter production, detoxification, and the regulation of homocysteine — an amino acid linked to cardiovascular health when levels get too high.How the Gene Works
The MTHFR gene provides the instructions for making this enzyme. Everyone has two copies of the MTHFR gene, one inherited from each parent. When the gene works normally, the enzyme efficiently converts dietary folate into its usable methylated form. Variants (sometimes called mutations or polymorphisms) in the MTHFR gene can reduce how efficiently this enzyme works.Reduced Efficiency Is Not the Same as Broken
Here is the critical nuance that gets lost in online discussions: reduced efficiency does not mean the enzyme stops working entirely. Even the most studied MTHFR variants only reduce enzyme activity by a percentage — your body still methylates folate, just somewhat less efficiently. Understanding this distinction is key to separating evidence-based health decisions from the fear-driven narratives that dominate MTHFR discussions online.The Two Major MTHFR Variants: C677T and A1298C
C677T (rs1801133)
Two specific variants in the MTHFR gene have been extensively studied. The first is C677T (rs1801133), located at position 677 of the gene. The "C" represents the common nucleotide (cytosine), and the "T" represents the variant (thymine). This substitution changes the amino acid at position 222 from alanine to valine, producing an enzyme that is thermolabile — meaning it loses activity more readily at higher body temperatures. C677T is the more clinically significant of the two variants.A1298C (rs1801131)
The second is A1298C (rs1801131), located at position 1298. Here the common nucleotide is adenine (A), and the variant is cytosine (C). This changes the amino acid at position 429 from glutamate to alanine. A1298C has a milder effect on enzyme function than C677T and is less well-studied in terms of clinical outcomes.How Common Are These Variants?
Both variants are extremely common. The C677T variant, for example, is carried by an estimated 35–45% of people of European descent (counting those with at least one copy), with allele frequencies tending to be higher in Southern European and certain Latin American populations. Having an MTHFR variant is normal human genetic variation, not a rare disease-causing mutation.Homozygous vs. Heterozygous: What Your Genotype Means
C677T Genotypes
- CC (wild-type): Full enzyme activity
- CT (heterozygous): One normal copy and one variant copy. Studies have estimated enzyme activity at approximately 65% of normal on average, though individual variation is wide.
- TT (homozygous): Both copies carry the change. Studies have estimated enzyme activity at approximately 25–35% of normal on average — enough for meaningful folate metabolism, but measurably reduced.
A1298C Genotypes
- AA (normal): Full enzyme activity
- AC (heterozygous): Mild reduction in activity
- CC (homozygous): Moderate reduction in activity
Compound Heterozygous
You can also be compound heterozygous, carrying one copy of C677T and one copy of A1298C (CT + AC). Research suggests this combination may have a modest effect on enzyme activity, somewhere between a single heterozygous C677T and a homozygous C677T. The key takeaway: only the homozygous C677T genotype (TT) has a consistently demonstrated clinical effect on folate metabolism and homocysteine levels. Heterozygous carriers and those with A1298C variants alone generally have little to no measurable health impact, especially with adequate dietary folate intake.MTHFR and Homocysteine: What the Research Shows
The Homocysteine Connection
The most well-established clinical connection for MTHFR variants is their effect on homocysteine levels. Homocysteine is an amino acid that is normally recycled back into methionine through a process that requires active folate. When MTHFR enzyme activity is reduced, this recycling can slow down, potentially leading to elevated homocysteine in the blood — a condition called hyperhomocysteinemia. Elevated homocysteine has been associated with increased cardiovascular risk, pregnancy complications (particularly neural tube defects), and potentially cognitive decline. However, the relationship is more nuanced than it appears.Folate Intake Makes a Big Difference
Studies show that homozygous C677T carriers (TT genotype) have homocysteine levels that are on average roughly 16–25% higher than CC carriers — though this elevation is most pronounced when folate intake is low. In populations with adequate folate intake (including countries with mandatory folic acid fortification of grain products, like the United States since 1998), the difference in homocysteine levels between genotypes shrinks significantly. This means that for many people with MTHFR variants, simply ensuring adequate folate intake through diet may be enough to keep homocysteine levels in a healthy range. A simple blood test for homocysteine can tell you whether your levels are actually elevated, regardless of your genotype.Folate, Folic Acid, and Methylfolate Supplementation
Folic Acid vs. Methylfolate
One of the most common questions about MTHFR is whether you should take methylfolate (5-MTHF) instead of regular folic acid. Here is what the evidence says. Folic acid is the synthetic form of folate found in supplements and fortified foods. It must be converted through several enzymatic steps — including the one catalyzed by MTHFR — to become active 5-MTHF. Methylfolate supplements bypass this conversion entirely, providing the already-active form.What the Evidence Says for Each Genotype
For homozygous C677T carriers (TT): there is reasonable evidence that methylfolate supplementation may be more effective than folic acid at raising blood folate levels and lowering homocysteine. Some clinical studies suggest methylfolate may be at least as effective as folic acid and possibly more beneficial for this genotype, though the evidence base is limited and the effect sizes in available trials have been modest. For heterozygous carriers (CT) or those with A1298C variants: the evidence for a meaningful benefit of methylfolate over folic acid is much weaker. Most heterozygous carriers process folic acid adequately.Practical Recommendations
For those with confirmed TT genotype and elevated homocysteine: your doctor may consider switching you to a methylfolate supplement (commonly in the 400–800 mcg daily range) as a reasonable, evidence-supported option. As always, supplement changes based on genetic data should be discussed with a healthcare provider. For everyone else, eating a folate-rich diet with plenty of leafy greens, legumes, and fortified grains is likely sufficient.Debunking MTHFR Myths: What the Internet Gets Wrong
Myth: "MTHFR Mutation Means You Can't Detox"
Reality: Methylation is one of many detoxification pathways. Even with reduced MTHFR activity, your body has redundant systems for processing toxins.Myth: "You Need an Expensive Methylation Protocol"
Reality: Most people with MTHFR variants need nothing more than adequate folate intake and possibly a basic methylfolate supplement. The elaborate supplement stacks promoted in some functional medicine circles have limited published clinical trial support and are generally not recommended by mainstream medical organizations.Myth: "MTHFR Causes Autism, ADHD, Depression, and Autoimmune Disease"
Reality: Statistical associations between MTHFR variants and these conditions have been reported in some studies, but the effect sizes are generally small, replication across studies has been inconsistent, and no causal mechanism has been established for most of these links.Myth: "MTHFR Is a Rare and Dangerous Genetic Mutation"
Reality: MTHFR variants are among the most common genetic polymorphisms in humans — researchers estimate C677T is carried by at least one copy in roughly 35–45% of people of European descent. High population frequency alone does not define risk, but it does mean these variants are a normal part of human genetic diversity rather than a rare, disease-causing mutation. The truth is that MTHFR variants exist on a spectrum, and for most carriers, they represent a minor metabolic variation — not a medical emergency.When MTHFR Variants Actually Matter Clinically
Pregnancy Planning
This is the most important scenario. Research suggests that women who are homozygous C677T may have a modestly increased risk of neural tube defects in their offspring, particularly when folate intake is inadequate — an association observed mainly in populations without mandatory folic acid fortification. For these women, preconception supplementation with methylfolate (rather than folic acid alone) may be a reasonable precaution, though standard prenatal folic acid doses are still protective for the vast majority.Confirmed Hyperhomocysteinemia
If a blood test shows elevated homocysteine and you are a TT carrier, your doctor can target the intervention more precisely.Methotrexate Therapy
This drug interferes with folate metabolism, and some oncologists and rheumatologists consider MTHFR status when dosing. This intersection of genetics and pharmacogenomics is an increasingly important area of precision medicine.What Major Medical Organizations Say
Beyond these scenarios, MTHFR genotyping is not currently recommended as a routine screening test by major medical organizations, including the American College of Medical Genetics and the American Heart Association. If you are curious about your status, it is worth checking — but it should be interpreted in the context of your actual health markers, not in isolation.Check Your MTHFR Status with DNA Explore
Private, Comprehensive, and Affordable
DNA Explore analyzes your raw file entirely in your browser — your genetic data never leaves your device, and no account is required. Beyond MTHFR, you will get a comprehensive analysis covering hundreds of health-relevant variants, pharmacogenomics (how you metabolize common medications), nutrigenomics, polygenic risk scores, and more. The full report costs $9.99 one-time, and you can preview a subset of results for free before deciding. If you do not yet have a DNA test, check out our comparison of the cheapest ways to get your DNA analyzed in 2026. Rather than paying for a standalone MTHFR test or relying on a wellness practitioner's interpretation, you can see your actual genotype, understand what it means in context, and share the results with your doctor if needed. Your genome data is already sitting in a file on your computer — DNA Explore helps you make sense of it privately, affordably, and based on the current scientific evidence.Frequently Asked Questions
Is having an MTHFR mutation dangerous?
Should I take methylfolate instead of folic acid if I have an MTHFR variant?
Can DNA Explore tell me my MTHFR genotype?
What is compound heterozygous MTHFR?
Do doctors recommend routine MTHFR testing?
Sources & References
Disclaimer: The information provided in this article is for general educational and informational purposes only and does not constitute medical, legal, or financial advice. Genetic information should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health decisions based on genetic data.
Prices, features, and availability of third-party products and services mentioned in this article are based on publicly available information as of the publication date and may have changed. We make reasonable efforts to ensure accuracy but cannot guarantee that all pricing, feature descriptions, or company information is current or complete. Trademarks and brand names referenced are the property of their respective owners and are used solely for identification and comparison purposes.
Genetic risk assessments, polygenic risk scores, and pharmacogenomic reports generated by any consumer tool — including DNA Explore — are based on currently published research and known associations. They are not diagnostic. Genetic predisposition does not guarantee the development or absence of any condition.
See what your DNA says about you
Drop your 23andMe or AncestryDNA file. Results in seconds. $9.99 to unlock everything.
Try DNA Explore freeAlready purchased? Restore your access